|
The American Heart Association Chain of Survival |
|
|
At the conclusion of this article you should be able to:
|
You awake to the alarm. This time it's not the obnoxious tones that punctuated your sleep last night; it's the alarm clock signaling the end of shift. It's time to go home and decompress after a hard night at the office.
You finish your paperwork while having that all important first cup of coffee. Finally, the oncoming shift assumes the position. You're in your car headed for home before the big hand hits the five.
Once at home, normal life takes over. You're now just another citizen. Your spouse is working on kitchen remodeling and needs to go to the mall to look at some appliances. You decide to tag along; it's a chance to get out and about. Your first stop is the store where America shops. You and your spouse wander through the appliances talking about what you want while looking for what actually fits your needs. Suddenly, you hear a commotion behind you. You turn to see a middle aged man lying on the ground, surrounded by people looking panicked. He isn't moving and his color doesn't look good. You think to yourself, "So much for a day off". You quickly cover the distance to the man on the ground and offer to help, identifying yourself as an off duty emergency worker. Someone tells you that the man just collapsed. You tell one of the bystanders to call 9-1-1 and then come back. The man is middle aged and lying motionless on the ground. You grab his wrist and check a pulse. Finding none, you check the carotid pulse and again, do not find one. As you quickly scan the area, you notice the familiar heart with lightning bolt symbol. You instruct one of the bystanders to go get the AED as you continue...
What is an Automatic External Defibrillator (AED)? Where did they come from and how do they work? How do they interface with EMS and why do I care? These are all important questions and will be answered in this article.
Back in the day when I was in paramedic school, the take home thought from the Advanced Cardiac Life Support (ACLS) section was "Live better with electricity". It seemed like the judicious use of electricity could solve all problems with cardiac arrest. The thought was to shock early, shock often, shock some more, shock again, and when the smoke cleared, start CPR. Defibrillation for the masses was still a concept. We were still considering whether to allow EMTs to defibrillate. Turning a defibrillator loose with the general population was still fiction.
Fast forward to today: defibrillation has come to the masses. Almost every shopping center in this country probably has an AED tucked away somewhere. Many businesses have added them to their safety programs. You should find them in most public buildings, especially arenas. They are now required on all commercial aircraft above a certain size. Amtrak is reported to have equipped most of their trains with AEDs. They may not be visible, but the staff will know where they are.
Many communities have started AED programs in conjunction with the local EMS provider, and AED training is part of many CPR classes. They realize how valuable AEDs and trained users are. Lives are being saved. Next time you are out and about, pay attention to the heart and lighting symbol that seems so common.
Humankind has always been fascinated with electricity. Over the ages electricity has progressed from being thought of as animal spirits to one of the most important commodities in the world. Electricity touches every aspect of our lives. In medicine the use of electricity has revolutionized cardiac care and contributed to the emergency medical services (EMS) that we know today.
The discovery that electric impulses stimulated and controlled muscle movements was first described in 1664 by Dutchman Jan Swammerdam.1 He proved that some muscle movements didn't involve the brain, disproving the connection between electricity and "animal spirits".
Sixty-one years later, the study of electricity had progressed to the point where Stephen Gray, an English scientist, identified conductors and insulators. His experiments with electricity showed that a charge could travel about 150 meters through wet hemp thread. He later concluded that the charge could travel even farther through a brass wire.1 The Leyden jar, or Leiden jar, is a device that "stores" static electricity between two electrodes on the inside and outside of a jar. It was invented independently by German cleric Ewald Georg von Kleist on 11 October 1744 and by Dutch scientist Pieter van Musschenbroek of Leiden (Leyden) in 1745-1746.1 The invention was named for this city. A French physicist, Jean-Antoine Nollet used that discovery to prove that electricity can travel through humans when he sent a charge of electricity through 180 of King Louis XV's Royal Guards.1
The first reference to using electricity as a cure for sudden death came in 1774. It was reported in the Annual Report of the Royal Humane Society that a three-year old girl had fallen out of the first story window of her house. After she was ruled dead by the attending Apothecary, it was decided to try electricity. Twenty minutes later the apothecary was able to finally apply the shock, "upon transmitting a few shocks through the thorax, he perceived a small pulsation: soon after the child began to sigh, and to breathe, though with great difficulty. In about ten minutes she vomited: a kind of stupor, occasioned by the depression of the cranium, remained for some days, but proper means being used, the child was restored to perfect health and spirits in about a week.' This success was repeated with chickens a year later. A lifeless hen was restored to life after a shock to the chest.1
Skipping ahead to 1849 we get the first documented case of Ventricular Fibrillation (VF) caused by a single electrical stimulus.2 Research during this time was aided by newer, more sensitive, instruments. Alexander Muirhead studied for his Bachelor of Science at University College London and then DSc (in electricity) at St Bartholomew's Hospital 1869-1872, where he is credited with recording the first human electrocardiogram. He said he didn't publish his work for fear of misleading others. The first documented EKG was published in 1887 by British physiologist Augustus D. Waller of St Mary's Medical School, London.3
The beginning of the twentieth century saw an increase in research related to EKGs. The first EKG was transmitted in 1905 by Willem Einthoven, who had coined the term electrocardiogram several years earlier, in 1893. The EKG was transmitted 1.5 km (4921 feet), from the hospital to his laboratory on March 22nd. Einthoven called the recording a telecardiogram. The next year Einthoven published the first presentation of normal and abnormal EKGs.1,3
The first esophageal EKG was achieved in 1906. The technique was first tested on a sword swallower. Esophageal EKGs became popular in the 1970s to differentiate atrial dysrhythmias, and were instrumental in the development of the AED. Another first for that year was the first fetal EKG transmitted through the abdominal surface.1
Originally, defibrillation consisted of plugging the machine into the wall. The voltage of the alternating current from the wall was transformed to between 300-1000 volts and was delivered via paddles directly to the heart.3 This technique was ineffective: the ventricular fibrillation usually returned. The morphology was different, representing cardiac muscle cell damage. These units were also very big, often requiring wheels to be moved. For this technology to become more useful, it would need to get smaller, lighter and more effective.
Development of better devices for measuring the electrical activity of the heart continued at breakneck speed through the first half of the twentieth century. As the equipment improved so did the diagnostic capability. Defibrillation continued to take a back seat to improvements in EKGs until 1947, when Dr. Claude Beck, successfully defibrillated a human heart during cardiac surgery.1,3 This open chest method proved that the concept could work, but was impractical for emergency use since it required direct access to the heart. Closed chest defibrillation was still a decade off. In 1956, Dr. Paul Zoll documented the first closed chest defibrillation, setting up what is now the standard for emergency cardiac care.4
The move to direct current began in the late 1950s with the work of Bernard Lown, M.D. Dr. Lown was looking for a better way to resuscitate those in cardiac arrest. Before the 1950s, the treatment of choice for people in cardiac arrest was drugs. Alternating current defibrillation improved patient outcomes, but was still unpredictable and left muscle damage. Dr. Lown was exploring using direct current. Instead of using a transformer, his plan was to charge a bank of capacitors to 1000 volts and deliver it at 100-200 joules. Dr. Lown filled a container with electricity and delivered it through paddles on the chest.5
Over time direct current replaced alternating current for defibrillation. The size issue remained. In order for this treatment to be effective a device needed to arrive quickly after someone presented with VF. Speed was of the essence as the chance of survival quickly diminished with the passage of time. Survival could be prolonged with cardiopulmonary resuscitation skills, but even with CPR the survival odds continued to diminish. Ambulance-transported Belfast physicians performed the first successful pre-hospital defibrillation in 1966, and three years later, EMTs without a physician on scene, did so in Portland, Oregon.6 Emergency cardiac care had effectively hit the streets. Following early success in Northern Ireland, defibrillators did get smaller, but were still heavy. Older devices weighed upwards of twenty-eight pounds. Models tested in England in the 1980s that used this technology not only monitored EKGs and defibrillated, but could also pace the heart.
As it became apparent that defibrillation was a life-saving necessity, the concern shifted to making it more available. The idea of a layperson defibrillating someone in cardiac arrest moved from fiction to fact. In the early 1970s, Dr. Arch Diack, Dr. W. Stanley Welborn, and Robert Rullman developed prototypes of AEDs. Instead of using two pads on the chest as with current models, they used one oral/epigastric electrode and a second electrode on the chest.6 Work continued, and in 1982 the US Food and Drug Administration (FDA) gave approvals for EMT-Defibrillation (EMT-D) clinical trials. Early trials were carried out in Washington, Iowa, Minnesota, and Tennessee. By the beginning of the 1990 reports of the successes were piling up, but there continued to be resistance to expanding the use of AEDs.
Studies continued, such as the one conducted by Dr. Roger White of the Mayo Clinic with the Rochester MN Police Department (RPD). Dr. White wanted to see whether police officers with AEDs could improve survival. Dr. White contacted the Rochester MN Police to see whether they would be interested in taking part in the study. RPD was very excited about the offer and quickly agreed to take part. RPD was already responding with Gold Cross Ambulance to all medical alarms, so this seemed a natural fit. RPD divided their city into four quadrants, each with an AED. They saw encouraging results over the first two years. Survival rose to 50%, a grand increase over the previous way of responding. The study continued, adding the Rochester Fire Department in 1998. The latest results from the study showed an overall 52% survival rate for witnessed VF.7
In 2004 the FDA began allowing AEDs to be sold without a prescription. This made them easier to acquire and helped their adoption within the community. There is still a large frontier waiting to be explored and conquered concerning defibrillation and AEDs. Homes are where most sudden cardiac arrests (SCA) occur, but are among the least effective places for AEDs. While AED use in homes is still under study, AEDS are now common-place. They are everywhere from the airlines to zoos.
The heart is a muscular double pump with four chambers that circulates blood to all parts of the body. It can be considered a double pump because it has a low pressure output, and a high pressure output. Since the lungs are in the same neighborhood as the heart, it doesn't take a lot of pressure to get the blood from the heart to the lungs and back. The right atrium, right ventricle, and the left atrium operate under this low pressure. The trick is to get the blood out to the rest of the body. That's where the left, high pressure, ventricle comes into play. The left side of the heart has bigger, thicker, muscular walls that, with contraction, can generate suitable pressure to move blood from the top of the head to the tip of the little toe. The remaining three chambers have thinner walls since they send the blood for shorter excursions. The chambers of the heart are separated by a thick wall of muscle and fibrous tissue which is called the septum. Across the walls of the heart are the conduction pathways that control heart muscle contraction. These conduction pathways are special muscle tissues that allow the impulses to be quickly conducted. These pathways conduct the impulses much more quickly than skeletal muscle tissue. The importance of conduction pathways becomes very evident when discussing the use of an AED.
The heart is unique in that it's innervated by both the vagus nerve and the cardiac plexus, but doesn't require direct action from the brain to function. The properties of automaticity in the muscle cells of the heart allow the cells to function autonomously. The brain does maintain control of the heart through nerve innervations, which may speed up or slow down the heart, but the heart still controls the beat. The heart functions with rhythmic clockwork accuracy to supply the body with the needed blood. The Sino-Atrial (SA) node, often called the anatomical pacemaker, is located in the right atrium. The SA node generates an impulse at a rate of 80-100 times per minute. As this impulse travels between the SA node and the Atrio-Ventricular (AV) node, the atria depolarize and contract. This so-called atrial kick stretches the ventricular walls to improve cardiac output by approximately 15%. After the impulse leaves the AV node, it travels into the bundle of His, then through the bundle branches and, finally, into the Purkinje fibers. During this sequence the ventricles depolarize and contract. Should something happen to the SA node, the AV node can assume pacing control with a rate of 40-60 times per minute. If that fails, the heart has yet another backup system. The next runners up are the ventricles, which take over at a rate of 20-50 bpm. The ventricular rhythm begins slowly, and then gets faster. The conduction center with the fastest rate controls the heart. To put this all into perspective, a "normal" conduction system will function at a resting rate of 60-100 beats per minute. The "normal" pacemaker is the SA node.
|
Defibrillation is a procedure that is designed to deliver a current of electricity through the chest to depolarize a section of fibrillating heart muscle. The hope is that normal impulse conduction will be restored. This is far different from the public's perception of "jump starting" the heart. A defibrillation actually stops the current electrical activity of the heart, by completely depolarizing the heart muscle. This clears the conductive pathways, with the goal of one of the normal pacemakers restoring organized electrical conduction. Still confused? We will explain this in detail. For now, compare this to an electronic device, such as a cell phone or computer. No matter what the manufacturers say, sometimes electronics "lock up". They are still "on", but they are making no logical sense of themselves. A good pull of the power supply stops all of the craziness, and the next power up magically restores the order. A defibrillation stops an unorganized heart so that the normal pacemakers can "reboot" the heart.
To fully understand AEDs and defibrillation, you must have an understanding of what depolarization is. Depolarization is an electro-chemical process. A resting cardiac muscle cell is considered polarized because there is a -90 mV difference between the inside and the outside of the cell. This difference, called the resting potential, is maintained by the work of the sodium-potassium pump. The pump helps keep the positively charged sodium ions on the outside, thus maintaining a higher gradient on the outside. Sodium and potassium ions both carry a positive charge and are called cations. Chloride ions carry a negative charge and are called anions. When the cell receives an impulse from the cardiac conduction system, the cell membrane changes its permeability allowing sodium to start rushing in through special channels. Following the sodium, albeit at a slower pace, is calcium, another cation. With calcium comes muscle contraction.
After depolarization or defibrillation, there is a period where nothing electrical can happen. This is called the refractory period. If the cells receive another impulse from a pacemaker, nothing will happen. During this period the electrolytes are reset and ready to go again. The first thing to be done is to shut off the sodium-potassium pump. With the cell in its charged state it will stay contracted forever. Once those pumps are shut down, special channels open allowing the potassium to rapidly bolt from the cell. Once the potassium channel closes, the sodium-potassium pump restarts to finish restoring the cell to its resting state.
As the repolarization begins, nothing will happen if the cell receives another impulse. But as the process continues, the cell enters a period called relative refractory period. If the cell receives a strong enough impulse during this phase, it will depolarize again. If the impulse isn't strong enough, the cell will continue to repolarize. A contraction that occurs during the relative refractory period will move blood, but it won't be as strong as a regular contraction.
When the pathology of cardiac arrest takes effect, the normal polarization and depolarization process described above goes awry. This leads to a condition called ventricular fibrillation (VF). This is an unorganized quivering of the myocardium. Another similar condition is ventricular tachycardia. Patients experiencing pulseless tachycardia will quickly deteriorate to ventricular fibrillation. Left untreated, these dysrhythmias will ultimately lead to asystole, the absence of electrical activity in the heart.8
|
If size and weight were the first revolution in the defibrillator world, wave forms and energy levels were the second. Defibrillation energy levels are a balancing act between having enough energy to get the job done and creating myocardial damage. It does little good to defibrillate at a lower energy level if that level isn't adequate to fully stop the heart and abolish the VF so that another pacemaker can take over. Disagreement over appropriate energy levels have helped drive the debate between monophasic and biphasic shocks.
Before comparing monophasic and biphasic any further, we must discuss energy levels. If you are like most EMS providers, you may have never heard of the term "joules" until learning about defibrillation. In electrical terms, voltage is a measurement of pressure. Watts and Joules are measurements of quantity. Joules differs from Watts in that a joule also measures time. Consider a hose or pipe flowing water. Volts would be equivalent to the pressure of the water flowing, such as 35 pounds per square inch. Watts would be equivalent to the amount of water that flows out of the hose, such as 10 gallons. Joules would be the equivalent to the amount of water flowing during a specific time frame, such as 5 gallons per minute. Therefore, the joules delivered in a defibrillation account for a number of watts, delivered at a certain voltage, over a specific time frame. That is about as deep into electricity as you need to go for this topic.
Early on, DC defibrillators were designed to deliver monophasic shocks. Monophasic defibrillation means that the current flow moves in one direction (polarity), from one paddle to the other. Early monitor/defibrillators were this type and it remained the workhorse of EMS for years. Many monophasic defibrillators and AEDs are still in service.
|
Biphasic Defibrillation occurs when the current alternates direction. The energy delivered flows from one paddle to the other for half the shock and then in the opposite direction for the second half. It was originally developed for implantable cardioverter-defibrillators. The theory is that using this type of waveform results in less energy needing to be delivered causing less damage to the heart and fewer skin burns. This technology has been around since the late 1980s and is incorporated into newer models of AEDs.
While all defibrillators and AEDs currently manufactured are biphasic, one must understand that the American Heart Association makes no recommendation of one over the other, neither type of waveform "is consistently associated with a higher rate of return of spontaneous circulation (ROSC) or rates of survival to hospital discharge after cardiac arrest".9
The range of biphasic shocks is generally 100 - 150, as opposed to monophasic shocks, which is generally of 200 - 360 joules. Studies have shown that a biphasic shock of 115 Joules is clinically equivalent to a 200 Joules monophasic shock. This is one of the reasons for the manufacturer switch to biphasic AEDs. Delivering lower powered biphasic shocks means improved battery life and quicker defibrillation charges in addition to causing less myocardial damage.
|
Studies have shown that the efficacy of the first shock of biphasic shocks is much higher than monophasic shocks. Efficacy is defined as the ability or capacity to produce an effect. Biphasic shocks were shown to have a greater than 90% success rate. One source puts monophasic AEDs in the neighborhood of 61%.10 Regardless of the type of AED used, the results pointed in the same directions. If the first shock doesn't convert, it probably means more CPR is needed, not necessarily more shocks.
Early protocols elevated the importance of the AED over CPR. As time passed and results started to pile up, protocols changed. Now the concept is that AED and CPR are on the same level of importance. The standards focus on the integration of CPR and AED use. The AHA recognizes that CPR alone won't likely eliminate VF and that the chances for survival with intact neurologic functions decrease much more quickly without CPR.
CPR and AED use must work hand in hand for patients to survive with intact neurologic functions. To increase the possibility of survival, three elements must be present. The first is the rapid recognition of a cardiac arrest and notification of the emergency medical services (EMS). The second is high quality CPR performed by a well-trained provider. The third is use of an AED. Neither CPR nor AED use is the sole solution. Some years ago the American Heart Association (AHA) started using the concept of the chain of survival, with each facet representing a link.
When someone in cardiac arrest presents, what do you do? Do you shock first, or start compressions? The answer to that depends on whether the arrest is witnessed or unwitnessed. "Witnessed arrest" can be thought of as a "really oxygenated arrest". In other words, if you get to the patient within a minute of the arrest, the heart is still relatively oxygenated. Why does this matter? Consider this scenario. You are working in the cardiac intensive care unit. The alarm goes off on a cardiac monitored patient. You run from the desk to the patient. Even though you did not visually watch the patient arrest, you were quickly alerted and arrived to the aid of the patient while the heart was still relatively oxygenated.
With a witnessed out-of-hospital arrest, the answer is to shock first if an AED is immediately available on site. The devil is always in the details. What does immediately available mean? In the case study above, you're at a shopping mall. The mall has an AED, but it's in the office. Does that mean immediate? It could be, if the office is next door and the round trip is about a minute. If the office is on the other side of the complex and someone has to get the key, then no, it's not immediately available. Whether something is immediately available or not could also depend on who has to retrieve it. If you are the sole responder, is your time better spent looking for an AED or doing CPR? We can "what if" this to death. Good sense has to come into play here: the rescuer must decide what is best for his or her patient.
If the arrest is not witnessed, what is the first step? The AHA standard puts CPR on point. The AHA recommends that the rescuers do two cycles of CPR before using the AED. This adds between 1.5 to 3 minutes (average - 2 minutes) of CPR before the use of the AED. The recommendation is backed up by two studies which showed that when EMS response is greater than 4-5 minutes, patients who received CPR before the arrival of EMS had a higher rate of initial resuscitation, hospital survival, and one year survival. This may not be the definitive answer since the AHA also considered a randomized study that concluded that there was no benefit to CPR before defibrillation for non-paramedic witnessed sudden cardiac arrest.11 The AHA also suggested that EMS medical directors consider implementing a protocol that would allow responders to provide five cycles of CPR before defibrillation for patients presenting in VF, especially if the response time is greater than 4-5 minutes.
AEDs are increasingly found in hospitals and other health care facilities such as doctors' offices. In these facilities, when an arrest occurs, CPR should be started immediately and the AED used as soon as it's available. The AHA supports early CPR and early defibrillation in health care facilities especially when the AED is available within moments of the sudden cardiac arrest.
The concept of a nurse grabbing an AED to resuscitate a patient in the hospital seems very foreign; after all, it's a hospital. With all the highly trained medical professionals and equipment available twenty-four hours a day, resuscitation shouldn't be a problem. Studies have shown the same basic results for sudden cardiac arrest in the hospital as outside the hospital. Instead of looking at response times of EMS professionals, they look at the arrival time of the designated code blue teams.
There are several types of AEDs in the field. Most are designed for lay rescuers to use. The AED provides guidance to the rescuer through all the steps. Some of the newer ones will even coach the rescuer through all the CPR steps and provide a metronome or other guidance to help keep CPR compressions at the right speed and depth.
Not everything that is called an AED is automatic; most of what is called an AED was really a semiautomatic external defibrillator. The difference between an automatic defibrillator and semiautomatic is the push of the defibrillate button. With an automatic defibrillator the machine does everything. You put on the pads, turn it on, and it handles everything. When it's finished, it tells you to start CPR. The semiautomatic prompts the user to stand clear of the patient and to use the shock button.
You may also run across regular monitor/defibrillators that have an AED mode. These allow both EMTs and Paramedics to use the same device. The AED mode makes the machine behave just like a standard AED. This increases its value to the emergency services community. One piece of equipment, two uses depending on how the selector switch is set. Some AEDs have additional features such as a "big brother" recorder that records everything that is said in addition to the time that various actions were taken. This information can then be uploaded to a computer and added to any medical records of the event.
|
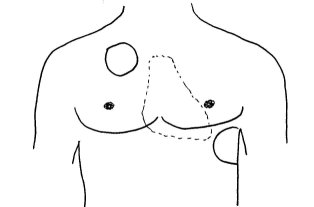
The primary goal of defibrillation is to deliver a current of electricity across a fibrillating myocardium in presence of little transthoracic resistance. Keeping that in mind, if a choice is available, the recommendation is to use self-adhesive defibrillator pads over paddles. The pads are safe and effective and alleviate some of the issues with paddle defibrillation such as paddle pressure.
Electrodes are placed on the patient's bare chest. Probably the most common placement pattern is the sternal-apical position, similar to the standard placement for paddles. In this placement the right patch is placed on the patient's chest right of sternum and below the clavicle bone. The left patch is placed on the left side lateral to the left breast. Another possible placement is the biaxillary method. This requires that the pads be placed on the right and left sides of the chest at breast level. This method is considered just as effective as the sternal-apical placement.
Placing the left pad in the apical position and the right pad on the upper back on the right or left side is another optional placement. One factor that may help you decide where to place the electrodes is the proximity of implanted medical devices. Implanted defibrillators and pacemakers are becoming common as development of these devices progresses. It is suggested that you place the pads about one inch (2.5 CM) away from the device. If the patient has an pacemaker or implanted defibrillator you should continue to use an AED as it is unknown if the implanted device is functioning correctly, just place the AED pads at least an inch away from the patient's device. You should suspect the presence of an implanted cardiac defibrillator (ICD) if you see a mass just under the skin close to the heart or see muscles twitching similarly to the way they would during an external defibrillation. ICDs typically will not discharge more than six times. A recurrence of VF/VT would be required before the unit will shock again.
Another factor to consider is the presence of transdermal medications such as nitroglycerin transdermal paste, hormone replacement patches, or nicotine patches. Do not cover the patch or paste with the defibrillation pad; it may block part of the charge, creating a burn. Remove the patch or paste with a gloved hand and wipe the area clean before proceeding with applying the defibrillation pads.
AEDs are mini computers that serve one function; they compare the electrical activity monitored against a library of recorded rhythms and deliver a shock if it's applicable. These computers have a high accuracy rating, but always defer to safety. If the AED has trouble detecting a rhythm, it will not advise a shock. These computers are always on the lookout for such things as 50 or 60 cycle interference, loose electrodes, spontaneous movement or poor electrode contact or other things that will affect the accuracy of the analysis.
Originally, AEDs were designed to look for heart activity is excess of 150 times per minute. Since AEDs can only measure the electrical activity, there was no way for the machine to determine if there was mechanical activity associated with the electrical activity. These machines also looked at the amplitude of the QRS complex. This method didn't lend itself well to recognizing fine ventricular fibrillation, which has very low amplitude. Newer AEDS use a variety of methods to analyze the electrical activity. The AED looks at various aspects of the morphology, power spectrum, and time away from the baseline. AEDs repeat these checks every two to four seconds. Their accuracy is 76-96% for VF and nearly 100% for non VF rhythms.6
An AED is essentially a one trick pony; as it will shock only rhythms like ventricular fibrillation and monomorphic or polymorphic ventricular tachycardia. AEDs are ineffective on asystole and other rhythms that are traditionally considered non-shockable. They also don't cardiovert or do synchronized shocks.
Old school emergency responders have had the pulse check following defibrillation drilled into their heads. Now the recommendation is to immediately return to CPR following the defibrillation. No more worries about doing chest compressions on top of a heart that is trying to contract. The AHA recommends five cycles of CPR (about two minutes) following a defibrillation prior to checking a pulse. One study showed that only 2.5% of patients had a detectable pulse after the first defibrillation.
The AHA Guidelines remove the initial “Look, Listen, Feel” step for assessing patients. Rescuers should immediately begin CPR if an adult patient is unresponsive and not breathing normally. The AHA stress the importance of early, uninterrupted chest compressions and highlights a “C-A-B” (Compressions – Airway – Breathing) sequence.
It is important to minimize interruptions. Do not delay or interrupt chest compressions to check pulse or rhythm. When more than one rescuer responds, one rescuer should ready the AED while the other rescuer performs chest compressions.
The AHA emphasizes that even untrained bystanders can help: simply “push hard and fast” on the center of the person’s chest or follow the directions of EMS dispatchers. Trained providers should still provide 30 compressions and 2 rescue breaths in order to improve outcomes, especially for pediatric patients.
Studies of the AHA standard showed that chest compressions were only performed 51% to 76% of the total CPR time.12 This meant that between a quarter and almost half of time the patient was pulseless nothing was being done to circulate blood. Compounding the issue is the well-known fact that chest compressions, while effective, aren't nearly effective at circulating blood as a properly functioning heart. So we have reduced cardiac output because of chest compressions and large gaps with no circulation at all because of pulse checks. This doesn't bode well for patient survival. It takes little time for the heart to use its supply of oxygen and metabolic resources during pauses.
The first shock has become very important. It is a balance between myocardial damage from the defibrillation against the damage from a prolonged cardiac arrest. Since monophasic AEDs/Defibrillators have a lower percentage of success than biphasic units it was decided to use a full power or 360 j shock with monophasic AEDs/Defbrillators. Making the first shock the best shock is critical. If you are not certain of what type of unit you have, use 200 J.
Another problem that became evident with stacked shocks is a higher incidence of AV block following defibrillation. These blocks seemed more likely to develop after two or three shocks at 320 Joules, less likely at 175 joules, and even less likely after only one shock. These AV blocks were reported to be transient and didn't affect survival to hospital discharge rates.
|
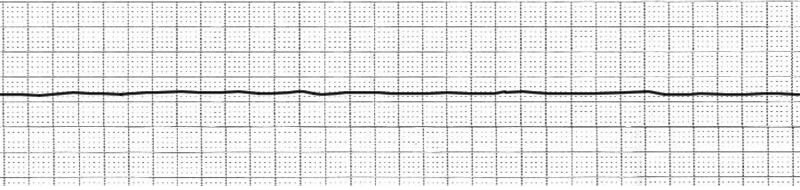
An AED will not shock all patients in cardiac arrest. Review the illustrations of the EKGs. An AED does not display the cardiac rhythm. The EKGs will simply help you to understand how the AEDs work. Ventricular Fibrillation and Ventricular Tachycardia show a course of up and down rhythm. These rhythms are what the AEDs are programmed to detect. Remember, a defibrillation shock is an attempt to stop the quivering muscle, so that an organized rhythm can be restored. Asystole is the absence of electrical activity, represented by the "flat line". Here, there is nothing to shock.
The EKG to the right looks like an EKG tracing of a normal heart. This is because it is! However, if the patient producing this tracing does not have a pulse, then the patient has pulseless electrical activity. In this case, the electrical impulses are being properly conducted, but the heart muscle is not contracting. Again, the purpose of a defibrillation shock is to restore an orderly rhythm. In this case, the absence of an orderly rhythm is not the problem. Therefore, an AED will interpret this, and advise no shock.
Problems with defibrillation using an AED are the same or similar to those when defibrillating using a standard monitor/defibrillator. Some of the problems are safety issues, and others relate to the pathophysiology of the procedure. Safety concerns for defibrillation need to be regularly addressed with drills, review classes, and safety articles. Whether the training is on AEDs as it is here, or regular monitor/defibrillators, safety issues should be reviewed.
If you are a fan of the television series House, you probably remember Dr. Kutner's prowess with the paddles. On one occasion, he sets the patient on fire after defibrillating him. On another, and more realistically depicted occasion, he pushed his way in with the paddles declaring, "He's dry enough", and promptly ended up on the floor; the patient wasn't dry enough. Defibrillation safety is more than just a slogan. There are a lot of elements that conduct electricity on an emergency scene. It could be the ambulance cot or the wet floor surrounding the pool. First and foremost, if you are going to be a "professional defibrillist" be aware of your surroundings before charging in or up.
Defibrillation can be hazardous for the patient too. The problems go beyond the obvious issues that come to mind when you introduce large quantities of electricity into the human body. One of the first concerns is skin burns; these commonly result from an inadequate quantity of electrolytes on the pads. The pads may be old and dry or were not stored properly. They may not stick to the body well, allowing air pockets to be forms which can result in arcing or burns. Paddles may not be gelled properly. Make sure the electrolyte gel is evenly distributed on paddles. If using electrolyte pads, make sure they are the right size for the paddle.
An issue with defibrillation that doesn't occur with most AEDs, but can be an issue with standard monitor defibrillators, is paddle pressure. Firm, downward pressure is required. Some old school texts state that you need twenty-five-pounds of pressure10 on the chest to ensure proper contact. Newer texts quantify the pressure as 8 kg, which is about 17.5 lbs. It is difficult to measure the amount of pressure applied. When you place the paddles on someone's chest, you do it for a purpose. Don't be hesitant. Be bold and forceful and the pressure issue will take care of itself. Another issue has to do with paddle or patch size. For adults, the proper patch/paddle size is thought to be 10 to 13 cm which is about 4 to 5 inches in diameter. In infants and children use the largest size possible as long as the pads or paddles don't touch. There should be at least 3cm between paddles.11
There are some physiologic problems related to defibrillation. The first one is the body's resistance to the conduction of electricity. Transthoracic resistance (impedance) is about 70-80 Ohms. If the body's resistance is too high, low energy shocks may have no effect.11 Men may be exceptionally hairy and may require shaving. Hair causes several problems when it comes to defibrillation or the use of AEDs. First, hair can cause excessive resistance to low energy shocks, which reduces the efficiency of the defibrillation. Hair can also prevent proper contact between the paddle or pad and the chest. Hairy chests can trap air and increase the possibility of arching or skin burns. Shaving the chest is always recommended except when it would excessively delay defibrillation.
Fire can be an issue when a defibrillator or an AED are used in an oxygen-enriched environment. Anything involving electricity has the possibility of creating a spark. Emergency service workers create oxygen enriched environments like ducks swim in water. They don't think about it; they just do it. Oxygen is usually one of the first interventions used on any sick or injured patient. When poorly applied defibrillator paddles are added, you have a recipe for a bad outcome. The use of self-adhesive defibrillator pads is recommended, but those pads are not always available.
Another solution is to use oxygen carefully. It is recommended that oxygen delivery devices are kept about three feet away from the chest when defibrillating. Devices can remain connected to endotracheal tubes or other airway adjuncts. Masks and cannulas should be removed and shut off or kept three feet from the patient's chest. Patients receiving positive end expiratory pressure (PEEP) may remain connected during defibrillation.
Cardiac arrest occurs less frequently in children. The causes of these cardiac arrests are typically related to hypoxia or trauma. Ventricular fibrillation as the presenting rhythm is also very uncommon, occurring in only about 5-15% of pediatric and adolescent arrests, but does increase with age. Many AEDs can be used under certain circumstances for pediatric patients. Some will recognize and differentiate shockable and non-shockable rhythms in all age groups; others require a key or specific pads for use with children. For children between 1 and 8 years of age, every attempt should be made to use an AED capable of delivering a pediatric-level shock. An AED with a pediatric mode, if available, should be used with children. If one is not available, the adult model should be used.
The American Heart Association categorized the use of AEDs in infants, those children between 0 and 1 year of age, as undetermined. AHA reported that there is insufficient data to determine the effectiveness of this procedure.11 One concern is whether interrupting CPR to detect if a rhythm can be shocked presents more risk than benefit.
The AHA Guidelines state that, "For attempted defibrillation of children 1 to 8 years of age with an AED, the rescuer should use a pediatric dose-attenuator system if one is available. If the rescuer provides CPR to a child in cardiac arrest and does not have an AED with a pediatric dose-attenuator system, the rescuer should use a standard AED. A manual defibrillator is preferred on infants less than 1 year of age. If a manual defibrillator is not available, an AED with pediatric dose attenuation is desirable. If neither is available, an AED without a dose attenuator may be used."13
As progress marches on, technology changes, and people adapt. Care for patients in sudden cardiac arrest is no different. From the early days where it was thought that animal spirits controlled body functions, through the experiments involving electricity and the heart, a much clearer indications have emerged of how the heart works and what to do when it doesn't.
Early defibrillators required wheels and plugged into the wall. Imagine how that would work in today's world. Imagine if one of your biggest concerns when treating someone in SCA was if someone had remembered to bring in the extension cord. We've moved forward from there. At first doctors on an ambulance used a defibrillator in Belfast. Now everyone from bystanders trained in CPR and AED to nurses in the hospital can use AEDs.
Good CPR and fast defibrillation are important partners in the fight against sudden cardiac arrest. The AEDs began as a way to give lay rescuers and those emergency service workers with little medical training a way to support the chain of survival. Studies show that every minute a person is in cardiac arrest their chances of survival quickly diminish. A tool that could analyze and determine whether a patient in arrest needed defibrillation and then could deliver it would save lives. AEDs were considered a fire extinguisher for cardiac arrest. They could help solve the problem, but the professionals still needed to finish job. Now the professionals are using that tool in places not originally anticipated. Nurses now call a code, graban AED and go to the patient's room. Instead of just doing CPR until the code team arrives, they use the AED to assess the patient's status and deliver defibrillation if needed. Nurses in hospitals and other medical facilities are now acting just like properly trained bystanders waiting for EMS or the fire department to arrive. Definitive cardiac care begins earlier and more quickly.
This improvement in the care of those in sudden cardiac arrest doesn't come without a price. There are risks to the operators of these devices and to those being cared for. Safety issues must always be first when using a device to defibrillate a person. The operator must ensure that the device is set up and used properly. Improper preparation or placement of the electrodes or paddles may lead to an unsuccessful first shock or unnecessary injury. To be able to effectively use a defibrillator or AED, it is important to understand how it works and how it affects the body. Understanding the anatomy and physiology of the heart along with the electro-chemical actions of depolarization and repolarization are important. Knowing that the refractory period is when the heart is unable to be depolarized and how the relative refractory period works are also important.
Waveforms and energy delivered are more than just setting on a machine. Biphasic AEDs and defibrillators have had more success at with lower joules than the old workhorse monophasic defibrillators. The amount of energy used is important since higher energy transmitted through the heart increases myocardial damage. The first shock is the most important.
AED use in children is new. The new standards now allow AEDs to be used on children in cardiac arrest. VF is an uncommon event in children. It is the presenting rhythm in only about 5-15% of all cases of pediatric cardiac arrest. Newer AEDs may automatically recognize if the patient is a child or require a key or special electrodes to change to pediatric mode. If no pediatric rated AED is available, use what is available, keeping the pads or paddles at least one inch apart.
AEDs and defibrillators are now a staple of emergency work. Staying up to date and practicing often is a must. There are no "do overs" in cardiac arrest.
Author Robert Provost, Copyright CE Solutions. All Rights Reserved.
References: